The Story That Changed My Thinking
(How My Granddaughter Changed My Thinking About What “Early Treatment” Means.)
“For years, I practiced orthodontics the way most orthodontists were trained. We evaluated around age seven. We monitored growth. We placed braces when it was time.
That changed when my three-year-old granddaughter began struggling with sleep.
She snored. She was restless. She was having trouble controlling her emotions and behaviors. Her development wasn’t following a normal pattern.
As I studied her structure, the width of her upper jaw, the way she was breathing (especially at night), and the posture of her tongue, something became clear to me.
Waiting was not neutral.
If I could see narrowing and airway limitation at three years old, why would I wait four more years to intervene?
That question forced me to rethink what “early” really meant.”— Dr. Bret Christensen
Dr. Christensen is a board-certified orthodontist with advanced training in dental sleep medicine, and every recommendation he makes is grounded in measurement.
The Data That Confirmed It
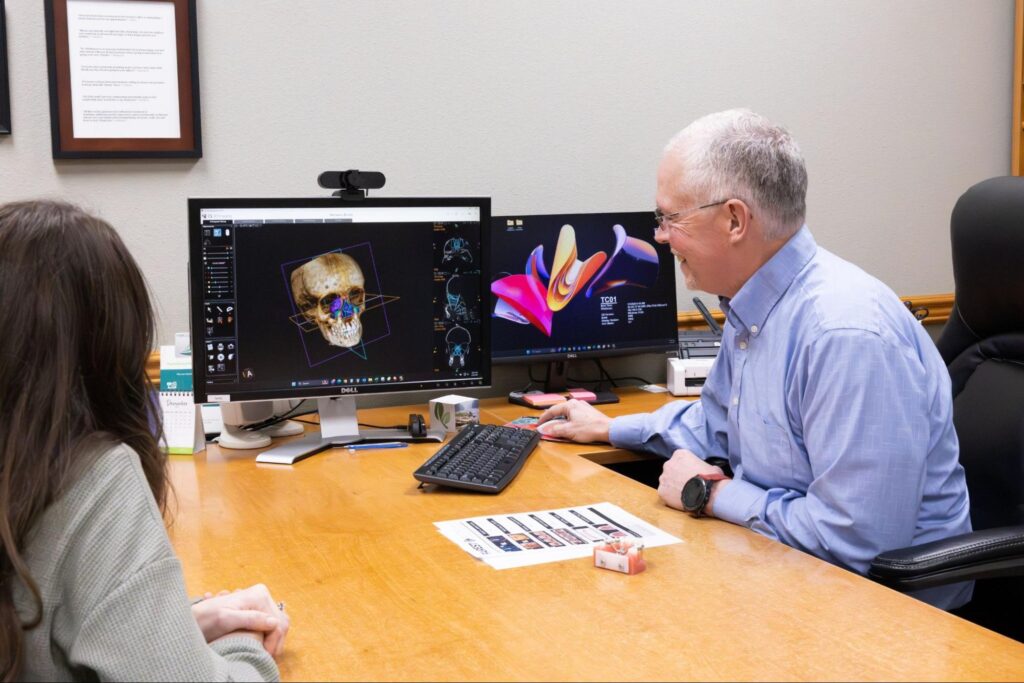
Since 2013, we have tracked airway and structural measurements in more than 340 cases using standardized CBCT and rhinometry protocols.
In pediatric patients, orthopedic expansion has produced:
- An average 42–46% increase in minimum airway size
- In some cases, nearly 100% improvement
- 4–6 millimeters of true nasal floor widening
- Measurable increases in nasal volume
This data has confirmed for us that when structure improves, nasal breathing often stabilizes. When breathing stabilizes, sleep quality frequently improves. When sleep improves, growth can proceed in a healthier pattern.
Early structural guidance is not cosmetic. It is foundational.
Why Waiting Is Not Neutral
The American Association of Orthodontists recommends orthodontic evaluation at age seven. That remains a reasonable baseline for general orthodontic screening.
But airway limitation does not wait until seven.
When a young child develops narrow jaws and unstable nasal breathing, growth follows that pattern.
Over time, this may contribute to:
- Early crowding
- Posterior crossbite
- Restless sleep
- Behavioral regulation challenges
- Jaw tension later in life
Waiting does not correct structure. Growth continues in the direction it is being guided.

What “Early” Actually Means
Early orthodontic treatment does not mean placing braces on toddlers.
In our practice, airway evaluation may begin at birth when tongue or lip ties affect feeding or breathing.
Structural guidance may begin as early as age three if measurable narrowing or airway restriction is present.
We do not recommend treatment based on age alone. We recommend it based on what can be measured.
What Happens If You Don’t Intervene Early
Without guidance, a narrow jaw does not simply catch up with growth.
- The upper jaw and palate can continue to narrow
- The nasal cavity and airway can constrict
- Tongue space can be limited
- The lower jaw may posture backward
- Permanent teeth may not have enough room to erupt properly
Improper facial growth tends to compound over time, reinforcing mouth breathing and shaping jaw development downward and backward.
What Happens If You Do Intervene Early
When growth is guided while the mid-palatal suture is still responsive, true skeletal widening is achievable.
Early palatal expansion can:
- Support forward facial development
- Increase nasal airway space
- Create room for permanent teeth
- Reduce orthodontic complexity later
The goal is not to treat early for the sake of treating early. The goal is to intervene when the data shows growth is off track.
How We Measure and Decide
We don’t guess.
As part of our Comprehensive Airway Evaluation, we measure:
- Palatal width
- Nasal floor width
- Minimum cross-sectional area
- Total nasal volume
- Mandibular position
- Tongue space and posture
Every recommendation is based on specific measurements and findings backed by data.
Airway Orthodontic Techniques We Use With Children
When measurements confirm underdevelopment, we guide growth at the level of bone.
The Everly Expander for Very Young Children
In children as young as three, we may use a pediatric expander designed for early skeletal guidance.
This device is banded to baby molars and activated gently to support jaw development and airway growth.
Rapid Palatal Expansion (RPE) for School-Age Children
A Rapid Palatal Expander widens the upper jaw at the natural growth seam to create true skeletal expansion.
Activation is controlled and biologic, not aggressive.
Guiding Forward Jaw Growth
Once the upper jaw is corrected, we may guide the lower jaw forward when needed.
The upper jaw leads. The lower follows.
Frequently Asked Questions
What age should my child see an orthodontist?
Evaluation is recommended by age seven, but airway concerns may be evaluated earlier.
Does every child need Phase One treatment?
No. Treatment is based on measurable findings, not age alone.
Can early treatment prevent braces?
Sometimes. It often reduces complexity and may avoid extractions.
Is age three too early?
Not if measurable restriction is present.
How do I know if expansion is needed?
We confirm this using objective airway and structural measurements.
The Next Step
If you are concerned about your child’s growth, breathing, or development, the first step is a Comprehensive Airway Evaluation at our Lewiston, Idaho practice. We measure structure, assess breathing, and then we decide together. We welcome patients from throughout North Central Idaho and from across the United States, Canada, and beyond.